iZafe Group AB (publ) has signed a letter of intent with Pilloxa AB regarding the acquisition of 100 per cent of the shares in Pilloxa. Pilloxa has developed a technology platform for better compliance that pharmaceutical companies use to design digital patient support. The acquisition creates a new company in digital health that is well positioned to become a leading player in better and safer drug use.
Incorrect or inadequate medication is a significant and costly problem for the individual and drug development companies and costs society substantial sums. Offering patients support to take their medication correctly is an effective way to achieve better medical outcomes. Both iZafe and Pilloxa today offer solutions that support patients in safe medical treatment. The merger means a broader and attractive offer to healthcare providers, the pharmaceutical industry and consumers, broadens the customer base and is expected to contribute to accelerated market penetration through clear sales and margin synergies.
– With Pilloxa’s digital offering and long-term collaboration with the pharmaceutical industry, together with iZafe, we can offer a comprehensive solution for our customers; patients, healthcare professionals and the pharmaceutical industry. Pilloxa’s promise to our customers today is a complete digital solution for patient support within one month of the initiation meeting. We are therefore used to rapid integrations and will immediately begin work on offering a joint digital solution, says Helena Rönnqvist, CEO at Pilloxa.
About Pilloxa
Pilloxa is a Swedish company that works to develop apps for patients to support them in adherence to their treatment and to connect patients, healthcare providers and the pharmaceutical industry. The company provides a SaaS platform where pharmaceutical companies and other customers can design digital patient support quickly, securely and at a low cost. Connected aids such as Pilloxa’s self-developed smart medication dose can also be connected to the service to support patients in taking the correct medication. Customers and partners include pharmaceutical companies such as Bayer Nordics and the Nordic office of Chiesi Global Rare Diseases, university hospitals such as the University Hospital in Oslo and universities such as the University of Gothenburg.
This article is the first in a series of pieces about Pilloxa and Sahlgrenska’s collaboration. Our Head of Marketing, Alexa Edstrom, sat down with research head Dr. Dimitrios Chantzichristos to discuss his upcoming research project and the use of digital components to support it.
When a curious researcher approached Pilloxa in 2021 about our solutions, we identified that we matched his research and data collection needs for an upcoming study he was hoping to conduct. Within the field of endocrinology, Dr. Dimitrios Chantzichristos and his team are working on finding answers for patients. Previous research has revealed treatment challenges in patients treated with both insulin and cortisone due to the opposing effects each has on glucose homeostasis and the need to adjust insulin treatment in relation to both cortisone and food intake in order to mimic the physiological endogenous profiles. If treated incorrectly, patients are at risk of developing hypo or hyperglycemia which can have serious consequences. No study to date has addressed this knowledge gap which affects those with diabetes and at the same time cortisone treatment because of Rheumatoid arthritis, asthma, different types of cancers, Addison’s disease and more.
Speaking with Dimitrios, I can see his clear passion for health. His inspiration to get into healthcare was because he wanted to serve people. He emphasizes the importance of listening to them, communicating with them, and ultimately helping them. He describes helping patients as putting together pieces in a puzzle, which has an investigative element he loves on top of the altruistic. Endocrinology, or the study of hormones, caught his interest due to the fact that so many endocrine diseases are diffused all over the body – all cells interact with the hormones in order for us to feel well.
Dimitrios studied his internal medicine specialization in Greece at the University of Patras, but came to Sweden to pursue a specialization in hormone diseases where he ultimately found a home-base for research and practice at Sahlgrenska University Hospital. At Sahlgrenska, he found many interesting patients with disease “puzzles” that were very intellectually stimulating to treat. It also gave him the chance to work with great colleagues, professors, and researchers within endocrinology. He tells me that he remembers the pure happiness he felt the day that Sahlgrenska offered him a long-term position, it was the perfect opportunity for him to do both clinical research and treat patients. Not only does Dr. Chantzichristos want to help patients in Sweden, he wants his research to help patients across the world and in the future.
Today, Dr. Dimitrios Chantzichristos is a Senior Consultant in endocrinology and Chief Physician at Sahlgrenska University Hospital. His previous research has covered topics such as hematologic diagnosis, biomarker discovery for cortisol effect in the body, and early indicators of Addison’s disease in type 1 diabetes patients.
His team’s upcoming research will involve patients with Addison’s disease, which their past research has also examined. Addison’s disease, also known as primary adrenal insufficiency, impacts patients due to their bodies not producing enough of certain hormones such as cortisol and aldosterone (source). Dr. Chantzichristos is very familiar with this patient group, as he works very closely with over 70 patients at his clinic in Gothenburg, Sweden. Many are open to participate in the upcoming study which is set to start in September of this year.
Digital components are essential to the study as the biggest challenge with these patients is to monitor many things at the same time. It is critical to measure fluctuations in dosing between treatments, when meals have been eaten, and other lifestyle factors. By using a continuous glucose monitor and Pilloxa’s solutions, successful data collection will hopefully be achieved.
The importance of this study is that its results will be relevant to all patients treated with both insulin and cortisone, which in Sweden alone is around 10,500 patients a year. The results will help shape recommendations on how to balance these two treatments in the presence of constantly changing factors such as timing of food, macronutrient distribution in food, physical activity, emotional stress and stressful events. By improving these treatments, the researchers believe that the risk of premature death that they have previously studied in this patient group will be reduced.
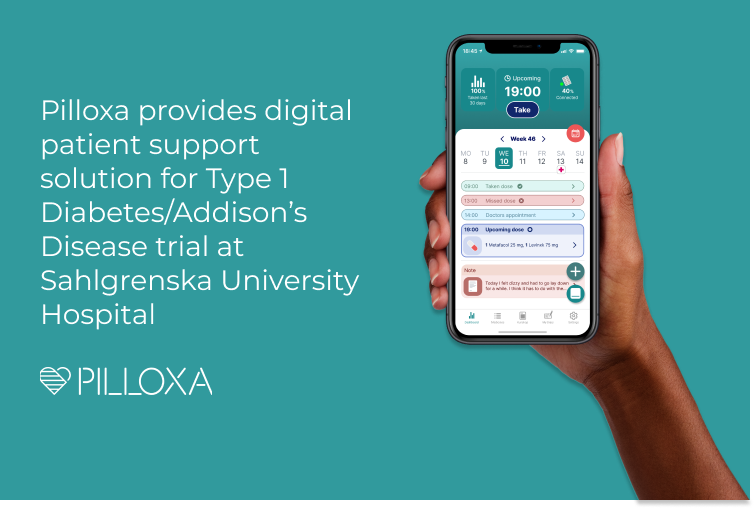
Stockholm, Sweden, April 26, 2022: Digital health company Pilloxa today announced they have signed a collaboration to provide a digital patient support solution based on their software and smart pillbox for a trial to be conducted at Sahlgrenska University Hospital involving patients with Type 1 Diabetes and Addison’s Disease. The project involves the Department of Endocrinology-Diabetes-Metabolism at Sahlgrenska University Hospital as well as the Department of Internal Medicine and Clinical Nutrition at the Institute of Medicine at Sahlgrenska Academy within the University of Gothenburg.
Patients suffering from both Type 1 Diabetes and Addison’s Disease are treated with both insulin and cortisone. This presents major challenges due to the opposing effects each treatment exerts on glucose homeostasis. Consequently, insulin treatment needs to be adjusted in relation to both cortisone and food intake to mimic the physiological endogenous profiles. Misalignment between factors such as timing of food, macronutrient distribution in food and physical activity can lead to emotional stress and stressful events including hypo- or hyper-glycemia, diabetic ketoacidosis, adrenal crisis and even death. The condition is not uncommon, in Sweden alone around 10,500 patients are treated with both insulin and cortisone a year.
Leading the collaboration with Pilloxa from Sahlgrenska is researcher Dimitrios Chantzichristos, M.D., who is championing research in the field by supporting these rare combination disease patients: “Patients with diabetes and cortisone treatment struggle in their everyday life to balance the doses of insulin and cortisone in order to avoid emergencies such as hypoglycemia and adrenal crisis. Our challenge as healthgivers is to provide them with efficient tools in order to minimize these risks. And this is the aim of our upcoming study, which wouldn’t be feasible without the use of modern digital health technology, as is so generously provided from Piloxa.”
The new trial seeks to advance understanding of the interplay between insulin treatment and intake of cortisone and food. Specifically, the aims are 1) to improve insulin treatment by identifying the periods with raised risk for hypo- or hyper-glycemia during the day and 2) to improve cortisone treatment by comparing the two available hydrocortisone tablet preparations in terms of metabolic and non-metabolic outcomes in patients with both insulin and cortisone treatment.
The research questions in the trial are the following:
Do patients treated with insulin & cortisone develop more often 1. hypoglycemia before the intake of cortisone tablets in the morning and 2. hyperglycemia during the evening compared with the rest of the day?
Do patients treated with insulin & dual-release hydrocortisone tablets have a more physiological cortisol profile and outcome compared with patients treated with insulin & conventional hydrocortisone tablets?
The researchers aim to answer these questions by studying glucose fluctuations in a well-defined patient group with insulin and cortisone treatment (patients with both type 1 diabetes and Addison’s disease) by collecting real-time information about the administration of insulin, cortisone, and food intake with the help of technology such as a patient app and continuous glucose monitor.
Pilloxa will support the trial with their software solutions and smart pillbox and Pilloxa’s CEO, Helena Ronnqvist, comments: “The importance of real-time data tracking and patient reporting is crucial for this study in order to establish recommendations on how to best medicate going forward as a patient taking both insulin and cortisone. We are proud to contribute to continuing research in this area and to support patients with both Type I diabetes and Addison’s disease. Managing medication daily alongside activities such as eating, exercising, work, and stressful events is not an easy feat and is complex to accurately track. We hope to make it easier by seamlessly fitting into a patient’s routine and providing the necessary data needed to develop their treatment journey.”
Ronnqvist continues: “With our digital patient support solutions, we aim to provide innovators with the needed tools and insights to enable sustained learning within health so that the focus can be shifted towards patient needs and how to best support them. Whether you are a researcher, doctor, or pharmaceutical company – you can use our solutions to better support your patients.”
This trial is scheduled to start in September 2022 with results by the end of 2023.
For more information, please contact:
Helena Ronnqvist, CEO, Pilloxa, .
Dimitrios Chantzichristos, MD and PhD, Sahlgrenska University Hospital, .
About Sahlgrenska University Hospital
Sahlgrenska University Hospital is one of Sweden’s largest hospitals. We improve healthcare through the application of strong innovation and clinic research in close and broad cooperation with academia, industry and patients.
The Faculty of Medicine at the University of Gothenburg. Research and education in medicine, odontology, and health and care sciences – always in close contact with practical care.
Pilloxa is a technological, regulatory, and legal platform for healthcare and pharma to create dynamic apps to support patients and learn from user data. Partners include Bayer, Chiesi, Sandoz, and Karolinska University Hospital.
To learn more about Pilloxa’s new product offering, explore our solutions at www.pilloxa.com
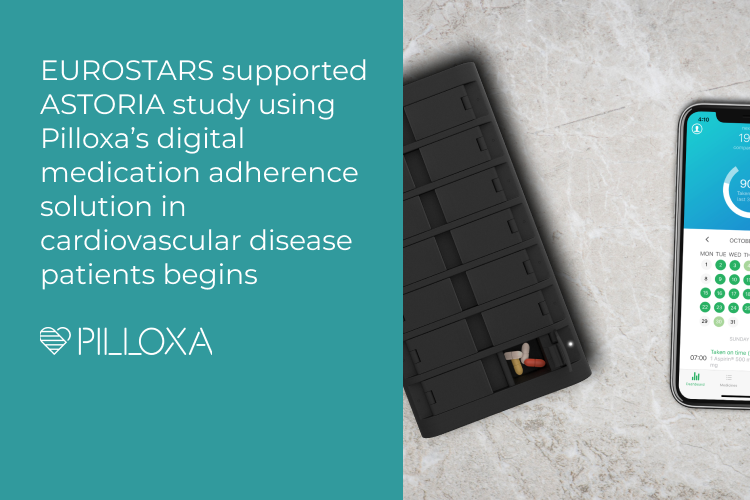
Stockholm, Sweden, March 9, 2022: Digital health company Pilloxa today announced that the First Patient First Visit milestone has been reached in the ASTORIA* study – a single-armed and multicenter observational clinical trial in which their digital patient-centric adherence solution is being tested in cardiovascular disease patients, namely newly diagnosed patients with atrial fibrillation. Professor Dan Atar from the University of Oslo is the sponsor of the study, financial support is provided by an EU-grant from the EUROSTARS program and Bayer.
The primary objective of the study is to assess the rate of adherence to rivaroxaban, an oral anticoagulant dosed once daily, in a study population of newly diagnosed atrial fibrillation using the Pilloxa box. Atrial fibrillation increases the risk of formation of blood clots in the heart and adherence to oral anticoagulants in patients with atrial fibrillation is of utmost importance to prevent the formation of these blood clots, that can be transported with the blood to the brain (causing stroke) and to other parts of the body. Non-adherence to medication increases the risk of hospitalization and mortality of patients, as well being a substantial economic burden for health care systems. The data gathered in this study will contribute to more knowledge on patient adherence, potentially with improvements in patient well-being.
The study will also further validate Pilloxa’s full suite of medication support services – including their adherence app enhanced with mobile communication and a digitally connected pillbox – to enable remote patient support. This includes alerting the patient to take their medication as prescribed and relaying their adherence patterns for further analysis. Furthermore, the results will likely enable further development of the Pilloxa solution in various other settings.
In the study, a dose of rivaroxaban for atrial fibrillation, taken from the Pilloxa medication dispensing box and measured by the adherence solution, will be considered adherent if taken on the same day as the planned dose (within a +/- 12 hour window). For additional, secondary endpoints, see below**. In total, 200 patients will be recruited and results from the trial are now estimated to be reported in 2024.
The principal investigator of ASTORIA, Dan Atar, Professor of Cardiology at the University of Oslo, comments: “We have reached an important milestone with inclusion of the first patient in the ASTORIA study. It will be interesting to see the impact that the technology supporting this trial has in supporting our patients with atrial fibrillation to take their anticoagulant medicines as prescribed. Data documenting whether patients have taken these medications as prescribed provides a good overview in real-time of patient adherence to medical treatment. It is anticipated that this knowledge will provide reassurance to the patient, relatives, and to the prescribing doctor. We also hope to learn how we can improve the quality of future clinical trials, a field in need of improvement when it comes to documenting the intake of drugs.”
Helena Ronnqvist, CEO of Pilloxa, states that: “This is an exciting milestone for everyone involved in the project, especially after the unexpected events of the past two years. We look forward to continuing to support patients with atrial fibrillation in adherence during their treatment journey with the potential to prevent complications and reduce the risk of medication side-effects. This trial will hopefully further demonstrate the effectiveness of using our software solutions and smart pillbox within the field, making it a breakthrough in patient support and drug intake documentation.”
* ASTORIA: ASsessment of Adherence TO Medication in AtRIAl Fibrillation – an eMonitoring Drug Dispensing Device Study
** Additional, secondary endpoints are:
Adherence will also be determined using the Norwegian Prescription Database, and a comparison will be made between the study population and a comparator population. For data from the registry, a Medication Possession Rate (MPR) of > 80% is considered to represent good adherence.
Rates of persistence and reasons for non-persistence
Risk factors for non-adherence and non-persistence in these patients, such as age, gender, socio-economic group, etc.
Patient-reported outcome regarding the use of the Pilloxa app and smart pillbox (ease of use etc)
For more information, please contact:
Helena Ronnqvist, CEO,
Cell phone: +46 707 995 159
About Pilloxa
Pilloxa is a technological, regulatory, and legal platform for healthcare and pharma to create dynamic apps to support patients and learn from user data. Partners include Bayer, Chiesi, Sandoz, and Karolinska University Hospital.
To learn more about Pilloxa’s new product offering, explore their solutions at www.pilloxa.com.
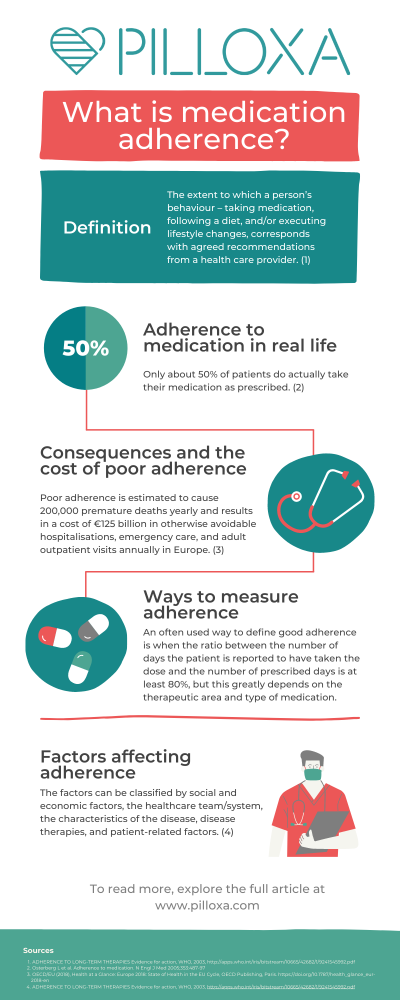
Adherence to medication is a term used to describe how well patients take their medication according to the plan created together with their healthcare professional. Sometimes it also includes adherence to other medical advice such as attending physical care, diet and lifestyle interventions, etc. The word adherence has come to replace the word compliance since it better captures the active rather than passive role of the patient. Several authors have tried to nail down a definition of adherence and the World Health Organization’s definition from 2003 is one of the most commonly used, defining it as “the extent to which a person’s behaviour – taking medication, following a diet, and/or executing lifestyle changes, corresponds with agreed recommendations from a health care provider” (1). It’s important to note that even though adherence describes a behavior occurring over time, the term persistence is used when referring to adherence over a long period of time.
In this article, we will explore how adherence is measured, what adherence means in the context of real life, factors influencing adherence, a few adherence solutions that are already available, and what the cost of poor adherence is to society as a whole.
What is “good” adherence and how is it measured?
What is good, moderate or poor adherence?
The fact that there is no universally well established definition of good, moderate or poor adherence makes the assessment of adherence and comparison between study results complicated. An often used definition of good adherence is when it is reported that a patient has taken their dose(s) correctly at least 80% of the prescribed days. Sometimes medicine possession ratio (MPR), the number of days the medicine is in the patient’s possession (collected from pharmacy), is used instead since this can more easily be tracked in registries. Again – 80% is often used as the threshold, however one should keep in mind that this threshold is arbitrary and does not directly relate to clinical relevance.
Direct methods
Direct methods to measure adherence include measuring the concentration of metabolites of the drug itself or the molecules added (markers) to the medicine solely for this purpose. Measures are usually made in blood, urine, feces, saliva or breath tests. This way to measure adherence is probably the most accurate. However, it has been hard to find a perfect marker to add to the drug for these kinds of measurements since absorbance and clearance patterns would have to be identical among subjects and not affected by diet, lifestyle, genetics, etc.
White coat adherence has also been described, i.e patients become more adherent and hence reach higher concentrations just before a doctor’s visits. Other disadvantages are the intrusive nature of taking the tests, the cost, the effect this testing has on the treatment alliance between the caregiver and patient, and that it is not practical in large scale, everyday treatment. Another direct method is direct observed treatment, DOT, where healthcare personnel or family members confirm the ingestion of a dose. These measures have been used in psychiatric settings and also in tuberculosis medicine in rural areas. A modern approach to this is the AI-confirmed ingestion, which solutions such as AI-cure utilize.
Subjective measures
Earlier, often used methods have been to let patients or care providers submit how medicine has been taken, for example, in paper or electronic diary form or in self estimation questionnaires. Several scales for this have been developed such as Morisky, BMQ and Hill-Bone. Unfortunately, subjective measures have many times been proven not to correlate very well with actual medicine intake but has been described as one of the least intrusive methods.
Objective measures
Pill count is probably the most used traditional method. Pills are then counted at a given moment, for example at the end of a study. This is compared to the number of pills the patient received from the start minus expected number of doses taken and the discrepancy indicates the level of nonadherence. This gives an idea of doses taken but of course there is no guarantee that the pills have actually been ingested or taken at correct dose times.
Secondary database analysis, for example analysis of refilled prescriptions compared to prescribed days as mentioned above, is sometimes used.
Electronic Medication Packaging (EMP) devices have been more commonly used and are by some considered the golden standard since the 1990’s. They often include a combination of features such as: (i) recorded dosing events and stored records of adherence; (ii) audiovisual reminders to signal time for the next dose; (iii) digital displays; (iv) real-time monitoring; and (v) feedback on adherence performance. The advantages of these devices are that they provide data about when the doses have been taken and that more work is needed to intentionally trick the device. Disadvantages are that it is often more costly, refilling needs to be addressed in some way, and some patients consider the box too chunky so they take out pills and store in other ways leading to false classification as non adherent (2).
A recent solution involves a sensor inserted in pills that is activated when ingested and thus delivers data about actual ingestion. This approach is of course harder to trick and it provides more accurate data. Drawbacks are the cost, the intrusiveness of the method, and usability since the user must wear a patch on their belly at all times.
Adherence to medication in real life
Chronic disease and health care spendings
Life expectancy is steadily increasing (3) and chronic disease is rising with it. In the EU, 100 million people living with chronic diseases medicate daily (4) and in the US 6 out of 10 adults have one chronic condition and 4 out of 10 have 2 or more (5). In 2017, countries in Europe spent on average 9.6% of GDP on health care, corresponding to an average spending of €2773 per person and the biggest spenders exceeded €4000 per person. On average, medicines accounted for 17% of total health expenditure (excluding medicines used in hospitals). In the US, 90% of the $ 3.5 trillion annual national health care expenditure was spent on people with chronic conditions and mental health conditions (6,7).
Adherence differences in populations
With this background, it is evident that a substantial part of the population is medicating on a daily basis and that astronomical resources are being spent on this. However, only about 50% of patients do actually take their medication as prescribed (8). Trials suggest that adherence levels vary between groups: for example adherence to antihypertensive medicine is ranging between 20-80 % (9,10). A primary nonadherence (meaning not filling the initial prescription) of 6-44% in asthma therapy has been demonstrated and secondary adherence has varied widely between 5-77%. Adherence to antidepressants also seems to differ greatly and 20-80% of patients have been reported not to follow prescription (11).
Even where therapies are more directly linked to saving lives, for example, after transplantation, poor adherence is reported among 20-50% of patients (12,13). Contrary to common beliefs, not only the elderly take medicine, there is a large group of younger people (aged 65 and below) with chronic diseases that medicate on a daily basis (14). Among them, nonadherence is a frequent problem, and some studies show that this group accounts for more missed doses than the older group (15,16,17,1,8,19,20).
Consequences and the cost of poor adherence
For the individual, poor adherence might have fatal consequences. It might, for example result in the loss of a transplanted organ or lead to stroke. Nonadherence to preventive cardiovascular medication increases the risk of hospitalization by 10-40% and the risk of mortality by 50-80% (21). Some studies suggest that up to 30% of people who seek emergency care is due to medical related problems (22) and an often cited number is that 10% of hospital enrollments are directly due to poor adherence (23). Poor adherence also causes worry among relatives, increases care utilization, and drives costs. In the US, nonadherence costs between $100-300 billion every year in healthcare costs alone (24). In Europe, poor adherence is estimated to cause 200,000 premature deaths yearly and results in a cost of €125 billion in otherwise avoidable hospitalisations, emergency care, and adult outpatient visits (25).
Factors affecting adherence
Traditionally, nonadherence has been viewed as something that is strictly related to the patient but over the last decades several factors have been identified as contributing to poor adherence. In 2003, WHO chose to divide these factors into: social and economic factors, the healthcare team/system, the characteristics of the disease, disease therapies and patient-related factors (26).
WHO states that “Patient characteristics have been the focus of numerous investigations of adherence. However, age, sex, education, occupation, income, marital status, race, religion, ethnic background, and urban versus rural living have not been definitely associated with adherence. Similarly, the search for the stable personality traits of a typical nonadherent patient has been futile – there is no one pattern of patient characteristics predictive of nonadherence.”
In recent years, focus has in some degree shifted back to individual forgetfulness and this has been acknowledged to account for a big part of the unintentional nonadherence (27,28). Pilloxa has explored the most common causes for medication nonadherence in our article here.
Adherence solutions
Several different approaches have been tried in order to tackle the widespread problem of poor adherence over the years. Often educational and informational interventions have been tried as well as individual and family therapy. Other approaches have been to simplify treatment regimens, to lower the cost for medicine, and to simplify the management of medication (e.g. pill organizers). For treatment monitoring, pill count has long been the golden standard whilst electronic monitoring has also become more frequent in recent years as technology has made it possible (29). Furthermore, reminders have gone from analog alarm clock reminders to be more advanced such as SMS text messages and calls.
In recent years, interest has increased in eHealth and mHealth (electronic and mobile health) and new solutions such as eMMD (electronic multi-compartment medication devices) and apps (mobile applications) have explored the opportunities within these fields. It seems that these newer electronic approaches have to some extent replaced old methods and are by some considered the new golden standard (ibid).
However, the clinical evidence that interventions do actually improve adherence and/or health outcomes vary in different studies. When it comes to analog pill organizers, studies show that these might increase adherence and outcome when used in some groups but results are inconclusive (30,31). Among older patients there was large room for improvement of usability factors in these devices (32), and possibly this lack of usability could in some groups lead to risks such as incorrect medication taking.
One large Cochrane review 2006 concluded: “For short-term drug treatments, counseling, written information and personal phone calls helped. For long-term treatments, no simple intervention, and only some complex ones, led to improvements in health outcomes. They included combinations of more convenient care, information, counseling, reminders, self-monitoring, reinforcement, family therapy, psychological therapy, crisis intervention, manual telephone follow-up, and other forms of additional supervision or attention. Even with the most effective methods for long term treatments, improvements in drug use or health were not large” (33). However, none of the reviewed studies included only an electronic monitor and reminder system.
A following Cochrane review in 2014 concluded: “…Across the body of evidence, effects were inconsistent from study to study, and only a minority of lowest risk of bias RCTs [randomized controlled trials] improved both adherence and clinical outcomes. Current methods of improving medication adherence for chronic health problems are mostly complex and not very effective, so that the full benefits of treatment cannot be realized…”. This review mostly included studies using informational/educational or therapeutic approaches (34).
Later reviews draw the conclusion that interventions, especially those including behavioural aspects and prompts to take medication, have an effect on adherence but that the effect on health outcome is unclear (35,36). Furthermore, there are some reviews that conclude that electronic reminders do have an effect on adherence (37) and two reviews show effect of electronic reminder systems on increased adherence indicating that this might be the new and possibly most promising kind of intervention to improve adherence (38,39).
We will most likely see a mix of analog, hardware, and software solutions as well as different strategies on tackling the issue at hand depending on the therapeutic area. It is great to have a variety of options to choose from since each patient population is different and requires tailored support to their unique needs. The end goal is to support patients in living better lives by improving adherence.
Conclusion and discussion
Poor adherence and how it relates to poor health outcomes and increasing cost of care has been known for a long time. It is evident that there lies a great opportunity to use health care budgets more efficiently if a solution to poor adherence can be found and implemented. It is rather surprising that a problem of this magnitude is still not addressed in a satisfying way in routine care.
Numbers of adherence rates are to be found in research but very few initiatives seem to be implemented to measure and track adherence rates in clinical practice. In some areas where concentration of drugs are being measured, for example within transplantation care, there is still no golden standard for improving adherence. Already in 2009 in the Nonadherence Consensus Conference Summary Report, this need was identified when one stated “the group also recommended that adherence monitoring be incorporated into the routine clinical management of all organ Tx recipients. Most importantly, it is imperative that such activity be reimbursed”(40).
Reasons for this might be the lack of direct financial incentives through reimbursement but also that there has been a challenge to find solutions that measure and address non-adherence in a correct way while also being acceptable from a user perspective, not too complex and intrusive and also cost effective.
It is clear that every person’s adherence pattern is a result of complex and highly individual underlying factors. It therefore seems reasonable that solutions aiming at improving adherence must be adapted and flexible around the individual behavior, disease, treatment, and other factors. Hopefully new technology with the capacity to analyze large amounts of data, and to create individually tailored responses, will be a gamechanger in patient support.
I believe that it is time to consider the end users not as “patients” but to acknowledge the fact that most of us will medicate for a chronic condition and that taking a pill a day does not change our priorities in life. Working, taking care of our loved ones, and engaging in activities will be taking up our time. Most of us do not want to spend more time than necessary on medicine rituals. Thus, for an intervention to be accepted it will need to flow seamlessly into our lives, providing more benefit than hassle. Complexity in the background but simple to the user seems to be a winning concept.
After decades of crushed hopes to see a widespread adoption of adherence solutions, maybe the COVID-19 pandemic will be the catalyst that finally drives this transformation in the medical space. It has accentuated the need for solutions to both facilitate and monitor adherence in home environments. New solutions are presented to the market at a rapid pace and it will be interesting to follow this development. Finally we also see a will to change reimbursement models that can fuel this change.
A very interesting question is, who will be the leaders driving this transition? Will it be healthcare providers and payers? New healthtech players? Or pharmaceutical companies seeking the opportunity to sell adherence as a service, e.g. in pay for performance models? It is clear that there is a massive opportunity for anyone who solves this problem in an efficient way and there is a risk of losing competitiveness for those that don’t and most likely we will see more and more collaborations between these actors.
– Helena Rönnqvist, CEO of Pilloxa
About Pilloxa
Pilloxa is a technological, regulatory, and legal platform for pharma to create dynamic apps to support patients and learn from user data. We provide innovators with the tools and insights to enable sustained learning within health so that our customers can focus on patient needs and how to best support them. Agile and affordable, pricing starts at €2500 a month and it takes only one month to launch a branded patient app with us.
Download
Our infographic below gives a great quick summary over the topic of medication adherence, download here.
Osterberg L et al. Adherence to medication. N Engl J Med 2005;353:487-97
Costa FV. Compliance with antihypertensive treatment. Clin Exp Hypertens. 1996;18(3-4):463-472
Cramer JA, Benedict A, Muszbek N, Keskinaslan A, Khan ZM. The significance of compliance and persistence in the treatment of diabetes, hypertension and dyslipidaemia: a review. Int J Clin Pract. 2008;62(1):76-87
Lennerling, A. & Forsberg, A. Self-reported non-adherence and beliefs about medication in a Swedish kidney transplant population. Open Nurs. J. 6, 41–6 (2012).
Denhaerynck, K. et al. Prevalence, consequences, and determinants of nonadherence in adult renal transplant patients: A literature review. Transpl. Int. 18, 1121–1133 (2005).
Henriksson J. et al. A Prospective Randomized Trial on the Effect of Using an Electronic Monitoring Drug Dispensing Device to Improve Adherence and Compliance, Transplantation. 2016 Jan;100(1):203-9.
Butow P. et al. Review of adherence-related issues in adolescents and young adults with cancer. JCO November 10, 2010 vol. 28no. 32 4800-4809
F. Dobbels et al. Adherence to the immunosuppressive regimen in pediatric kidney transplant recipients: A systematic review, Pediatric Transplantation, Volume 14, Issue 5, pages 603–613, August 2010.
Age-related medication adherence in patients with chronic heart failure: A systematic literature review., Kreuger et al., Int J Cardiol. 2015 Apr 1;184:728-35. doi: 10.1016/j.ijcard.2015.03.042. Epub 2015 Mar 4.
The impact of age and gender on adherence to antidepressants: a 4-year population-based cohort study, Amir Krivoy et al., Psychopharmacology (Berl). 2015 Sep;232(18):3385-90. doi: 10.1007/s00213-015-3988-9. Epub 2015 Jun 21.
Medication adherence in HIV-infected adults: effect of patient age, cognitive status, and substance abuse, Charles H. Hinkin et al., AIDS. 2004 Jan 1; 18(Suppl 1): S19–S25.
Ho PM et al, Medication adherence: its importance in cardiovascular outcomes. Circulation 2009; 119(23):3028-3035
Fryckstedt J. et al. Läkemedelsrelaterade problem vanliga på medicinakuten, LÄKARTIDNINGEN, 2008-03-18 nummer 12
Iuga, A. O., & McGuire, M. J. (2014). Adherence and health care costs. Risk management and healthcare policy, 7, 35–44. https://doi.org/10.2147/RMHP.S19801
Konstadina Griva, Ph.D., Andrew Davenport, FDRC, Michael Harrison, FDRC, Stanton P. Newman, Ph.D.Non-adherence to Immunosuppressive Medications in Kidney Transplantation: Intent Vs. Forgetfulness and Clinical Markers of Medication Intake 2012, Annals of Behavioral Medicine, Volume 44, Issue 1, August 2012, Pages 85–93, https://doi.org/10.1007/s12160-012-9359-4
Khan MU, Shah S, Hameed T. Barriers to and determinants of medication adherence among hypertensive patients attended National Health Service Hospital, Sunderland. J Pharm Bioallied Sci. 2014;6(2):104‐108. doi:10.4103/0975-7406.129175
Adams R, May H, Swift L, Bhattacharya D. Do older patients find multi-compartment medication devices easy to use and which are the easiest? Age Ageing. 2013 Nov;42(6):715-20. doi: 10.1093/ageing/aft113. Epub 2013 Aug 26.
Conn VS1, Ruppar TM2. Medication adherence outcomes of 771 intervention trials: Systematic review and meta-analysis. Prev Med. 2017 Jun;99:269-276. doi: 10.1016/j.ypmed.2017.03.008. Epub 2017 Mar 16.
Vervloet M1, Linn AJ, van Weert JC, de Bakker DH, Bouvy ML, van Dijk L. The effectiveness of interventions using electronic reminders to improve adherence to chronic medication: a systematic review of the literature.Journal of the American Medical Informatics Association, DOI: http://dx.doi.org/10.1136/amiajnl-2011-000748 696-704 First published online: 1 September 2012
R.N Fine, Becker et al, Nonadherence Consensus Conference Summary Report DO – 10.1111/j.1600-6143.2008.02495.x American journal of transplantation : official journal of the American Society of Transplantation and the American Society of Transplant Surgeons
Swedish digital startup company Pilloxa today announced that it is to collaborate with the Nordic office of Chiesi Global Rare Diseases on using the Pilloxa platform to support the treatment journey for patients with nephropathic cystinosis across Scandinavia.
Nephropathic cystinosis is an ultra-rare, multisystemic, genetic disorder characterized by the accumulation of the amino acid cystine in the lysosomes within the cells. This accumulation leads to damage in various tissues and organs of the body including kidneys, eyes, muscles, liver, pancreas and brain (1). The continuous progression of the disease, together with the high medication burden, places large demands on the patients and their caregivers. Most younger patients, under 11 years of age, follow the prescription correctly. (2) However, as with other chronic diseases, many teenagers, and young adults with nephropathic cystinosis are struggling to follow the treatment regimen. Strategies such as better information on the disease, patient self-care promotion, and facilitated transition to adult healthcare services have been suggested to improve compliance and the clinical management of cystinosis. (2)
With the app Cool 2B Rare_C we are aiming at helping patients to take control of their disease and treatment. In the app, patients and caregivers, such as family members, will be able to:
set reminders on when to take the medication
follow the adherence over time
have easy access to information about the disease and related topics.
“We are honored to work with the Nordic office of Chiesi Global Rare Diseases to support patients, an incredible partner within rare diseases aiming to improve the lives of people across the world. Digital solutions have a great potential to give personal support to chronically ill patients at every step on the treatment journey, to give hope and motivate them in their everyday battle. Together we are at the forefront of a new paradigm within personalized healthcare, and we are just getting started. We strongly believe that this will increase the quality of life for patients with nephropathic cystinosis and hope to ease the transition of care into adult life for many patients,” commented Helena Rönnqvist, CSO Pilloxa.
“Our approach is to develop and test solutions that we believe will benefit patients, caregivers and health care professionals in diagnosing patients early as well as managing a rare or ultra-rare disease. We look forward to receiving feedback on this app from the nephropathic cystinosis community.” Patrick Svarvar, Head of Rare Diseases, Nordics Chiesi Global Rare Diseases
“Patients are the beginning and the end of our journey. In the work developing this app, Pilloxa has interviewed patients, caregivers and physicians to get an insight on the gaps that need to be filled in order to improve the treatment journey. We would like to thank all of them for giving their time as well as sharing their knowledge on how it is to live with nephropathic cystinosis.” Brita Forsberg, Medical Advisor, Nordics Chiesi Global Rare Diseases
About Chiesi Global Rare Diseases
Chiesi Global Rare Diseases is a business unit of the Chiesi Group established in February 2020 and focused on research and development of treatments for rare and ultra-rare disorders. The Global Rare Diseases unit works in collaboration with Chiesi Group to harness the full resources and capabilities of our global network to bring innovative new treatment options to people living with rare diseases, many of whom have limited or no treatments available. The unit is also a dedicated partner with global leaders in patient advocacy, research and patient care. For more information visit https://www.chiesiglobalrarediseases.com/
About Chiesi Group
Based in Parma, Italy, Chiesi is an international research-focused pharmaceuticals and healthcare group with over 85 years’ experience, operating in 30 countries with more than 6,000 employees (Chiesi Group). To achieve its mission of improving people’s quality of life by acting responsibly towards society and the environment, the Group researches, develops and markets innovative drugs in its three therapeutic areas: AIR (products and services that promote respiration, from new-born to adult populations), RARE (treatment for patients with rare and ultra-rare diseases) and CARE (products and services that support special care and consumer-facing self-care). The Group’s Research and Development centre is based in Parma and works alongside 6 other important research and development centres in France, the U.S., Canada, China, the UK, and Sweden to promote its pre-clinical, clinical, and regulatory programmes. Chiesi, since 2019, is the world’s largest B Corp certified pharmaceutical group. The global B Corp movement promotes business as a force for good. The Group is committed to becoming carbon neutral by the end of 2035.
Chiesi was established in the Nordic region in 2014 and has operations in Sweden, Denmark, Norway and Finland.
The founders started Pilloxa after their Clinical Innovation Fellowship program in May 2014. The confusion and worry in patients following their treatments sparked their passion and they saw that their combined background in technology, medicine, and entrepreneurship could bring high impact. Stockholm proved to be a unique hub due to its presence of world leading healthcare organizations and access to top global talent. From their first steps with the Karolinska University Hospital to current partnerships with sector leaders, Pilloxa is now a European sector leader rooted in the Scandinavian peninsula.
To learn more about Pilloxa’s new product offering, explore their solutions at www.pilloxa.com
References
Elmonem et al. Orphanet Journal of Rare Diseases (2016) 11:47
Ariceta et al. Nephrol Dial Transplant (2015) 30: 475–480
Press Questions? Please contact Alexa Edstrom at or +46 76 567 3713 (Sweden)
Stockholm, Sweden, June 3rd, 2021: Digital health company Pilloxa today announced the launch of their new product offering, a cloud-hosted solution for pharmaceutical companies and medical research teams to engage patients and learn from them. Through creating branded programs within Pilloxa’s patient-facing mobile app, the customer can provide patients with a customized experience for a fraction of the average cost while generating valuable data insights. Pilloxa’s new product offering will innovate the market with standardized pricing to fit patient support programs and clinical research budgets of all sizes.
Pilloxa’s platform allows the customer to become the innovator themselves and accelerate patient-centric learnings. Through the platform, the customer chooses the modules that they would like to include in their own patient-facing mobile app program, including medication support, adherence dashboards, and even interactive learning material on the medication and treatment journey. The customer also provides the content, allowing them to fully brand the material to the extent they wish and allowing them to form a valuable relationship with patients. If the customer wishes to further support adherence for patients with medication in pill form, Pilloxa’s original smart pillbox can still be connected to the app as well.
“Creating your own program within the integrated Pilloxa mobile app establishes a link to patients to provide value and collect data for driving innovation,” explains Pilloxa CEO Francesco Mazzotta. “By analyzing engagement within the patient-facing app through Pilloxa’s web interface, the customer can iterate as often as they like by making changes to the app to deliver value and become the leading expert on their unique patient population. Furthermore, all patient functionality is always included and new modules are constantly introduced – to ensure patient value throughout the lifespan of the program”.
Further innovating their vertical within their industry, Pilloxa is clear in their standardized, flat-fee pricing. The customer pays for what they use and there are no hidden costs. To further aid customers, all processes and documentation are standardized and transparent to assist with faster internal processes when working with regulatory and legal departments.
Pilloxa has already built up a strong network of collaborators. Pharmaceutical partners include Bayer Pharmaceuticals in Sweden and Sandoz Pharmaceuticals in Scandinavia, while medical research partners include the University of Oslo, Karolinska University and Hospital, as well as Danderyd Hospital. Pilloxa has also received EU innovation funding alongside investments from top Swedish investor profiles.
Together with their new product offering, Pilloxa is also launching their new brand identity as well as a new website. Their new branding includes a more refined color palette hinting at their Scandinavian heritage while still incorporating elements from their past brand. The website also now includes an interactive pricing calculator and app visualizer for customers to play around with what solution would best fit their needs and budget.
Speaking on the importance of unlocking the innovation potential in Life Science, Pilloxa CEO Francesco Mazzotta wants to remove barriers to innovation within the industry while never compromising on patient value when democratizing innovation.
“We have seen the need for innovation within the industry and the willingness of pharmaceutical companies and research institutions to facilitate change, however many blockers remain. Connecting apps with medication taking is no longer a question. It is about creating value for patients and delivering optimal health solutions. No company within healthcare will stay relevant without that. User response will be the guiding light to understand in which way to combine them on a case by case level, and the impact will be felt by all stakeholders involved within the patient journey.”
To learn more about Pilloxa’s new product offering, explore their solutions at www.pilloxa.com
About Pilloxa
The founders started Pilloxa after their Clinical Innovation Fellowship program in May 2014. The confusion and worry in patients following their treatments sparked their passion and they saw that their combined background in technology, medicine, and entrepreneurship could bring high impact. Stockholm proved to be a unique hub due to its presence of world leading healthcare organizations and access to top global talent. From their first steps with the Karolinska University Hospital to current partnerships with sector leaders, Pilloxa is now a European sector leader rooted in the Scandinavian peninsula.
Questions? Contact or call our Head of Marketing, Alexa Edstrom, at +46 76 567 3713
Stockholm, Sweden: Digital health company Pilloxa today announced the start of ASTORIA* – a single-armed and multicenter observational clinical trial in which their digital patient-centric adherence solution will be tested in patients with cardiovascular disease, namely newly diagnosed patients with atrial fibrillation. The study, to be conducted as a multicenter trial with the University of Oslo as lead, is funded by an EU-grant from the EUROSTARS program and is also financially supported by Bayer. The aim is to further validate Pilloxa’s full suite of medication support services – including their adherence app enhanced with mobile communication and a digitally connected pillbox – to enable remote patient monitoring. This includes alerting the patient to take their medication as prescribed and relaying their adherence patterns for further analysis. The data gathered will enable further development of the solution to increase the quality and effectiveness of drug treatment in both the healthcare setting and during clinical trials. In total, 200 patients will be recruited and results from the trial are estimated to be reported in 2022.
The primary endpoint of this study is adherence to rivaroxaban as measured by the Pilloxa adherence solution. A dose will be considered adherent if taken on the same day as the planned dose (within a +/- 12 hour window). For additional, secondary endpoints, see below**.
The principal investigator of ASTORIA, Dan Atar, Professor of Cardiology at the University of Oslo, comments: “Patients with atrial fibrillation carry an increased risk of developing serious and life-threatening events, a stroke being the most common. Fortunately, modern oral anticoagulant medicines have been shown to lower this risk, but it is of utmost importance that the patients take their medicine as prescribed. In the current trial, patients will be reminded when they need to take their medicine and relevant information around the treatment (e.g. time when the medicine was taken) will be automatically documented. Data documenting whether patients have taken these medications as prescribed provides a good overview in realtime of patient adherence to medical treatment. It is anticipated that this knowledge will provide reassurance to the patient, relatives, and to the prescribing doctor. We also hope to learn how we can improve the quality of future clinical trials, a field in need of improvement when it comes to documenting the intake of drugs.”
High adherence to anticoagulation treatment in atrial fibrillation patients is important for the prevention of thromboembolic complications and to reduce the risk of side-effects from the medication. Despite this, data has shown that patient adherence to their new oral anticoagulation (NOAC) medication gradually drops to 60% when evaluated after the first 12 months of treatment. Ensuring that patients take their medicine as prescribed is crucial as the effect of this new medicine on coagulation in the blood cannot be measured.
“That adherence to treatment is fundamental for any therapy to be successful is easy to accept but our research has shown that in practice, adherence is poor in many cases. The advantage of our technology, which we have developed and documented over the last 5 years, is that it can be added as a new layer without changing the organization, running intensive training programs or making new, expansive investments”, says Francesco Mazzotta, CEO of Pilloxa. “Another advantage is that using our system does not bring any burden onto the patient. Contrary to being a burden, it helps the patient to carry out the treatment in an easier and more efficient way. Patients also tend to be more engaged, and the automatic documentation enables efficient feedback with minimal administration between healthcare providers and the patient, a truly patient centric solution.”
Francesco Mazzotta adds: “If the study shows improved adherence rates with the use of Pilloxa, this would provide a strong argument for such devices to be implemented routinely for atrial fibrillation patients with an indication for use of long-term treatment with oral anticoagulant. Furthermore, a positive result would also speak in favor of using Pilloxa’s solution in conjunction with treatment with other drugs where adherence rates to medication is central for enhanced outcomes. Given the importance of adherence to treatment for reliable testing of drug effects in early phase clinical trials, we are continuously exploring such investigations with industry partners.”
* ASTORIA: ASsessment of Adherence TO Medication in AtRIAl Fibrillation – an eMonitoring Drug Dispensing Device Study
** Additional, secondary endpoints are:
Adherence will also be determined using the Norwegian Prescription Database, and a comparison will be made between the study population and a comparator population. For data from the registry, a Medication Possession Rate (MPR) of > 80% is considered to represent good adherence.
Rates of persistence and reasons for non-persistence
Risk factors for non-adherence and non-persistence in these patients, such as age, gender, socio-economic group, etc.
Patient-reported outcome regarding the use of the Pilloxa app and smart pillbox (ease of use etc).
All of us have forgotten to take a pill. We are human and make mistakes. Some of us neglect to take our medication for accidental reasons, while for others it may be intentional. So, what are the main causes of medication non-adherence? By better understanding the causes, we can work to provide solutions for our patients that better support them along their journeys. The causes of nonadherence can be managed to reduce the risk of the patient not taking their medication. Let’s dive deeper into the causes to explore what continues to drive medication non-adherence.
1. Forgetfulness
Just like implementing any new habit, incorporating the act of taking medication into your daily routine can be a challenge at the start. It requires reminders, accountability, and drive to stay consistent. Even for veteran medicators, a change in environment or schedule can throw off their routine and lead to missed doses. It’s human nature to forget things, even when things have become routine. Perhaps a new medication even alters your memory capabilities, which is why reminders are vital along our medication journeys – to support us when we most need it.
2. Fear and Worry
As a patient, it’s common to have anxiety around new medication, perhaps around expected side effects or the social stigma of taking medication in public. This may result in a patient intentionally not taking their medication and then fearing to tell the truth to their healthcare provider. By educating the patient on their condition, their upcoming journey, how to cope with side effects, and the importance of their medication – they can be better supported to overcome any fears or challenges they may face. Medicine myths can be rejected and the patient can make more educated decisions, empowering them to have more constructive consultations with their doctor addressing their concerns. The right knowledge at the right time is extremely important.
3. Misunderstanding
What a medicine is prescribed for, how the medication should be taken (e.g. together with a meal or not), and for how long the medication should be taken is information that can often be misunderstood or misinterpreted between doctor and patient. It has actually been shown that only 49% of all patients remember the instructions given after a visit (see here) not to mention what this number is after a few weeks. This is one of the most common causes of poor adherence, and unsureness of how to take a medication might result in the patient not taking it at all, medicating in the wrong way, or even medicating in excess which could result in avoidable side effects. Ensuring that the patient has easy and accessible information to revisit when needed is an easy way to reduce this cause. Many of today’s smart solutions also offer feedback systems that present information that might be of interest for that individual based on behaviour patterns. When a patient fails to see results after some time, they may become non-adherent despite the medication needing to be taken for longer in order for you to start seeing true results. It is important to continuously educate the patient on their condition and medication to continue to build trust and support them when needed.
4. Adverse side effects
For many, the side effects of a new medication may be too negative or intense to wish to continue being adherent. Similar to fear and worry, a patient may intentionally stop taking their medication due to the side effects. It is important to report any adverse side effects and to discuss with a doctor how to manage side effects that will appear along the way and when it is time to change medication if they become too negative. Ensuring that adverse events can be easily and quickly reported, while also continuing to educate patients of the natural course of side effects and potential, serious side effects is crucial.
5. Complex medication schedules
Complex medication schedules require supporting your medication organization in addition to having set reminders to take doses throughout the day at the right time intervals. For some patients, such as minors, others may have to be involved to support the patient in medicating. Accountability helps a patient stay on track, so incorporating support from a partner or caretaker is beneficial. Adding in reminders that a prescription has run out can also further support patients to stay proactive and support their adherence.
6. Lack of symptoms
It has been shown that it is particularly difficult to maintain a medication taking behaviour when the medicine is of preventive nature. If a medication is taken to avoid an event in the future and when the patient does not feel any direct positive effect from taking the medication or direct negative effect from not taking the medication it is of course even harder to keep the motivation high. Imagine the difference in short term motivation in taking painkillers when having a headache versus cardioprotective treatment that might prevent a heart attack in 15 years. The course of such non-adherence usually starts with missing one pill… and without any negative feedback then a few more doses are missed leading to maybe a whole week without medication – thus the behavior of taking medicine is broken and medicine taking stops. Lack of side-effects or taking medication in a preventive nature does not equate to being healthy. Again, this further illustrates the point of why continuously educating patients is beneficial.
7. Suffering mental health
If a patient suffers from a mental illness which negatively alters their mental state, this can impact a patient’s ability to take their medication on schedule and as prescribed. Mental health support along a patient’s journey is key to ensure that they can feel the best they can to actively contribute to their own treatment. Therefore, empowering a patient with the knowledge of when to seek help, if they need it, can be crucial
How can we tackle these causes?
Medication adherence has always been a problem, but today we are fortunate to have cutting edge technological solutions to curb an increase in medical nonadherence paired with healthcare systems that are dedicated to improving their quality of care and treatment.
First and most easily, we can support medication organization and reminders easily by using apps on our phones and a simple pill organizer. Different people prefer different organization styles, but an old school pillbox and setting reminders always helps.
Secondly, we can work to facilitate better relationships between healthcare providers (HCPs) and patients so that they feel there are open communication channels and that they can express their concerns and what hesitations might keep them from taking their medication as prescribed. This also ties into helping to clear up misunderstandings, which can be further supported by clear information and instructions for patients regarding their medications that are always accessible. Supporting mental health also plays a role here, as we can check in on patients who are struggling in order to help them and ensure they stay adherent through tough times.
Third, when it comes to symptoms and side effects, this is where information and clear communication channels between the doctor and patient is again crucial. Patients need to be well versed in what they should expect during their medication journey, and how they can best deal with negative side effects and how to evaluate if they are too risky for taking the intended medication. There should be trust between the two parties, but especially towards the doctor as they have the patient’s wellbeing in mind. If a patient can easily record their side effects, this allows them to report back to their doctor if they are facing issues that need to be addressed. Empowering them with knowledge allows them to have more constructive and beneficial conversations with their healthcare provider.
Fourth, incorporating psychology into how technological solutions are shaped to tackle medication adherence can help to keep users motivated using elements of empowerment, continuous support, and gamification. This includes using positive language and reinforcement, displaying their performance in a gamified way to encourage them to stay on track, and possibly even reaching out to them when they need extra support as identified by trigger actions and behaviors in-app.
There is a need for an actor, utilizing technology, to bring together the stakeholders of this important problem. At Pilloxa we hope to be that actor and provide better solutions to patients who need it. Patients like you. Patients like all of us. Until then, an open conversation with your doctor about adherence concerns can often lead to more effective solutions and improved safety, confidence, and well-being. By being aware of the top causes of medical non-adherence, we can holistically work towards solving this issue and ensuring better lives during treatment for our patients.
The importance of medication adherence in healthcare and how it impacts society. Written by Helena Rönnqvist, Chief Science Officer at Pilloxa.
The “western” world is a knowledge-based world. We have let go of religion, instead championing data and science as the correct and single source of truth. We believe in the individual and health as central concepts in our lives. We all attempt to be healthy. We walk 30 minutes a day, because someone at some point said that this improves health. We eat fruits and greens, because apparently that will help us too. Staying in good health is something that truly occupies our minds and time.
Yet, science showcases that there is no way to neglect the most evident fact of them all: we will all die. It’s a morbid truth. And it will happen rather soon when compared to the entire existence of the earth.
In a knowledge-based world, we are not sure if there is a second chance at life in heavenly paradise or a raging hell, and who knows what could happen with the potential of cloning research. To ensure that we live for a bit longer, or in our mindset, do not die, we spend a lot of time trying to avoid the unavoidable. We do many things to ensure a long life. We start working out, we eat healthy, and try to sleep well – since everyone knows that with less than 7 hours of sleep every night the risk of dying from cardiovascular disease doubles. If we feel a lump somewhere, we go to check it so that, if it turns out to be cancer, we can get treatment to avoid a worst case scenario. Despite our efforts, we all age and many of us reach a point where medicine becomes a part of our daily diet. We take pills to lower this risk and in essence prolong our lives and/or increase our livelihoods.
Society firmly believes in this. We believe it so much that society actually considers it a human right to receive medical treatment (as we should). In 2017, countries in Europe spent on average 9,6% of GDP on health care, corresponding to an average spending of €2773 per person. Sweden was one of the biggest spenders, spending €4019 per person. On average, medicines accounted for 17% of total health expenditure (excluding medicines used in hospitals). These massive spendings are often justified by cost/benefit calculations referred to as health technology assessments, known as HTA for short.[1]
“Do you take every pill as you are prescribed to? I know I don’t.”
All taken together, taking medicine seems to be a subject of very high interest both on an individual as well as collective level.
When I worked within the emergency ward at Karolinska Hospital in Sweden, it became clear to me that even though many of us have decided to start a treatment, it is not at all certain that we will properly follow or complete it. In many cases, that was the main reason as to why many of my patients were spending their day in the emergency bed in front of my eyes. Some studies suggest that up to 30% of people who seek emergency care is due to medical related problems [2] and an often cited number is that 10% of hospital enrollments are directly due to poor medication adherence [3].
At a first glance, this may seem very strange and paradoxical but when scratching the surface it becomes clear that taking medicine as prescribed is not at all a simple task.
Do you take every pill as you are prescribed to? I know I don’t. And you and I are not alone. Adherence to therapies is 50% [4] on average. Even where therapies directly save lives, for example after transplantation, poor adherence is reported among 20-50% of patients [5, 6]. Furthermore, contrary to common belief, the younger population appears to have the hardest time following their prescriptions [7, 8, 9].
Why is that? A very low percentage of the younger population suffers from cognitive impairment and most of them can at least theoretically understand why medicine is important to take. They have even put in the effort to visit a physician and undergone the discomfort of examination and testing to get that prescription.
Is it because thinking of how to improve health has finally become too much? Or do the pills in some way remind us of this inevitable thing called death? Maybe we just don’t like the touch or taste of the pills? Maybe it’s a mix of all of those reasons and more. Maybe none of them.
“There are so many reasons for why that pill is not taken out of its box, placed on the tongue, and swallowed.”
But above all of this, there’s this wonderful thing called life. And life can get in the way. One thing that ill people often witness is that when becoming ill it is not death but life that becomes more present. Maybe the rituals performed to prolong life lose some of their meaning and instead living the rest of life as fully as we can becomes more important to us.
And living a full life involves a lot of activities. There’s a lot of things to do: dinners with loved ones; concerts and cinemas to attend; trips and adventures to be experienced; kids needing to be played with; and there’s friends and family to see. Somewhere between all of this “life stuff” we have to squeeze in taking medicine. It can be such a mundane task to do. There are so many reasons for why that pill is not taken out of its box, placed on the tongue, and swallowed.
But the truth is not a hard pill to swallow in this case.
Most reasons to not take medication are not deliberate. It is more of a mishmash of reasons like forgetting to take the medicine, forgetting if you already took it, forgetting to collect it from the pharmacy, lacking routine, forgetting to renew the prescription, or maybe even the information of how or when to take your medication is uncertain. If, in the beginning, taking medicine might seem like a great idea in most cases there is no instant reward of doing so, and with time motivation declines. There might even be side effects that you need to struggle with, possibly making it even easier to let it fall into oblivion.
This of course leads to a lot of sad and avoidable health effects. For the individual, this might have fatal consequences. For example, it might result in losing a transplanted organ or leading to stroke. In Europe, poor adherence is estimated to cause 200,000 premature deaths yearly and results in a cost of EUR 125 billion in avoidable hospitalisations, emergency care, and adult outpatient visits [1].
Even though this problem has been known for decades, finding the right solution has been hard. It has been proposed that to overcome this massive problem one has to work with a multifaceted approach built around the individual rather than a population [10].
“Even though it seems like a hard nut to crack, the most promising thing about this problem is that there are no losers if the problem gets solved – only winners.”
Whose responsibility is it to solve this enormous problem? The individual who we so strongly believed in? Society that has put up a rigid structure of how to provide these potent drugs and also pays for much of the use or pharmaceutical companies that claim to sell medicine that improve health? Today, initiatives are being made from the state, clinics, patient organisations and industry. However, the outcome of these initiatives are rarely connected to direct reimbursement and the direct monetary incentives seem to be lacking even though the bill for non-adherence is in the end ultimately paid by taxpayers. Maybe if pay for performance models for medicine become more common we will see larger efforts, but that’s another topic to dive into.
Even though it seems like a hard nut to crack, the most promising thing about this problem is that there are no losers if the problem gets solved – only winners. And with emerging technologies, there is more hope than ever that multifaceted solutions directed to the individual really can make a change.
So to answer the question: does medicine really work? Only if you take them. As Haynes and colleagues well put it back in 2001: “Increasing the effectiveness of adherence interventions may have a far greater impact on the health of the population than any improvement in specific medical treatments” [11]. Therefore, it’s time to fit your medication seamlessly into your life so that you can focus on enjoying it.
And then, maybe we can trick death a little while longer…
Helena Rönnqvist, Chief Science Officer at Pilloxa
References
[1] OECD/EU (2018), Health at a Glance: Europe 2018: State of Health in the EU Cycle, OECD Publishing, Paris. https://doi.org/10.1787/health_glance_eur-2018-en.
[2] Fryckstedt J. et al. Läkemedelsrelaterade problem vanliga på medicinakuten, LÄKARTIDNINGEN, 2008-03-18 nummer 12.
[3] Iuga, A. O., & McGuire, M. J. (2014). Adherence and health care costs. Risk management and healthcare policy, 7, 35–44. https://doi.org/10.2147/RMHP.S19801.
[4] Osterberg L et al. Adherence to medication. N Engl J Med 2005;353:487-97.
[5] Lennerling, A. & Forsberg, A. Self-reported non-adherence and beliefs about medication in a Swedish kidney transplant population. Open Nurs. J. 6, 41–6 (2012).
[6] Denhaerynck, K. et al. Prevalence, consequences, and determinants of nonadherence in adult renal transplant patients: A literature review. Transpl. Int. 18, 1121–1133 (2005.
[7] Age-related medication adherence in patients with chronic heart failure: A systematic literature review., Kreuger et al., Int J Cardiol. 2015 Apr 1;184:728-35. doi: 10.1016/j.ijcard.2015.03.042. Epub 2015 Mar 4.
[8] The impact of age and gender on adherence to antidepressants: a 4-year population-based cohort study, Amir Krivoy et al., Psychopharmacology (Berl). 2015 Sep;232(18):3385-90. doi: 10.1007/s00213-015-3988-9. Epub 2015 Jun 21.
[9] Medication adherence in HIV-infected adults: effect of patient age, cognitive status, and substance abuse, Charles H. Hinkin et al., AIDS. 2004 Jan 1; 18(Suppl 1): S19–S25.
[10] WHO, ADHERENCE TO LONG-TERM THERAPIES: EVIDENCE FOR ACTION, 2003.
[11] Haynes RB. Interventions for helping patients to follow prescriptions for medications. Cochrane Database of Systematic Reviews, 2001, Issue 1, 2001.







{kind=link}